This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I'm Dr F. Perry Wilson of the Yale School of Medicine.
When I was doing my nephrology training, I had an attending who would write notes that were, well, kind of funny. I remember one time we were seeing a patient whose first name was "Lucky." He dryly opened his section of the consult note as follows: "This is a 56-year-old woman with an ironic name who presents with acute renal failure."
As an exhausted renal fellow, I appreciated the bit of color amid the ongoing series of tragedies that was the consult service. But let's be clear — writing like this in the medical record is not a good idea. It wasn't a good idea then, when any record might end up disclosed during a malpractice suit, and it's really not a good idea now, when patients have ready and automated access to all the notes we write about them.
And yet, worse language than that of my attending appears in hospital notes all the time; there is research about this. Specifically, I'm talking about language that does not have high clinical utility but telegraphs the biases of the person writing the note. This is known as "stigmatizing language" and it can be overt or subtle.
For example, a physician wrote "I listed several fictitious medication names and she reported she was taking them."
This casts suspicions about the patient's credibility, as does the more subtle statement "he claims nicotine patches don't work for him." Stigmatizing language may cast the patient in a difficult light, like this note: "she persevered on the fact that… 'you wouldn't understand'."
This stuff creeps into our medical notes because doctors are human, not AI — at least not yet — and our frustrations and biases are real. But could those frustrations and biases lead to medical errors? Even deaths? Stay with me.
We are going to start by defining a very sick patient population: those admitted to the hospital and who, within 48 hours, have either been transferred to the intensive care unit or died. Because of the severity of illness in this population we've just defined, figuring out whether a diagnostic or other error was made would be extremely high yield; these can mean the difference between life and death.
In a letter appearing in JAMA Internal Medicine, researchers examined a group of more than 2300 patients just like this from 29 hospitals, scouring the medical records for evidence of these types of errors.
Nearly 1 in 4 (23.2%) had at least one diagnostic error, which could include a missed physical exam finding, failure to ask a key question on history taking, inadequate testing, and so on.
Understanding why we make these errors is clearly critical to improving care for these patients. The researchers hypothesized that stigmatizing language might lead to errors like this. For example, by demonstrating that you don't find a patient credible, you may ignore statements that would help make a better diagnosis.
Just over 5% of these patients had evidence of stigmatizing language in their medical notes. Like earlier studies, this language was more common if the patient was Black or had unstable housing.
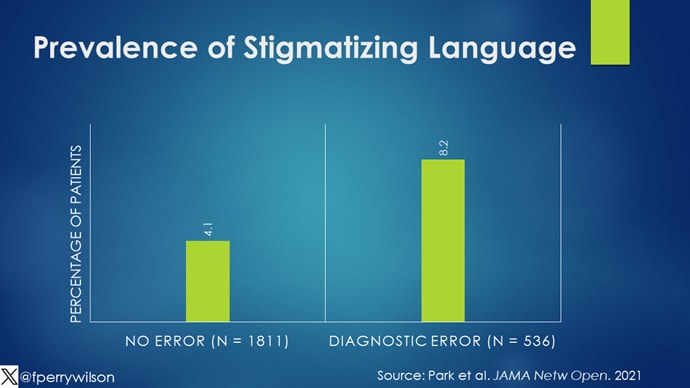
Critically, stigmatizing language was more likely to be found among those who had diagnostic errors — a rate of 8.2% vs 4.1%. After adjustment for factors like race, the presence of stigmatizing language was associated with roughly a doubling of the risk for diagnostic errors.
Now, I'm all for eliminating stigmatizing language from our medical notes. And, given the increased transparency of all medical notes these days, I expect that we'll see less of this over time. But of course, the fact that a physician doesn't write something that disparages their patient does not necessarily mean that they don't retain that bias. That said, those comments have an effect on all the other team members who care for that patient as well; it sets a tone and can entrench an individual's bias more broadly. We should strive to eliminate our biases when it comes to caring for patients. But perhaps the second best thing is to work to keep those biases to ourselves.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale's Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his book, How Medicine Works and When It Doesn't, is available now.
"difficult" - Google News
April 16, 2024 at 04:23AM
https://ift.tt/bdAw3e2
'Difficult Patient': Stigmatizing Words and Medical Error - Medscape
"difficult" - Google News
https://ift.tt/5hMNzF8
https://ift.tt/ADT8R4Y
Bagikan Berita Ini














0 Response to "'Difficult Patient': Stigmatizing Words and Medical Error - Medscape"
Post a Comment